

Ciheb's Digital Platform for Reporting and Monitoring QI Activities
Providing quality healthcare in resource-constrained settings is a challenging undertaking. Yet, even in these environments, methods to regularly monitor the quality of care exist. Developing a set of quality indicators between healthcare providers, patients, healthcare leaders, and the community, collecting and analyzing data on those indicators, identifying gaps, and co-designing solutions create a platform for continuous quality improvement (CQI) efforts.
In Tanzania, health facilities, with support from various implementing partners, have been using different approaches in the design, process, monitoring, and reporting structures of quality improvement initiatives. The Ministry of Health, Community Development, Gender, Elders and Children (MOHCDGEC) realized the need to have a standardized approach to providing quality HIV/AIDS health services. Tanzania Quality Improvement Framework (TQIF) was developed for the first time in 2004. A quality improvement guideline for HIV/AIDS services based on strategies and actions from the TQIF was later developed in 2009. Both of these documents have had several updates since then. Current versions can be found here.
The goal of CQI is ensuring that the services provided are of supreme quality and contribute toward optimum patient and program outcomes. There is a greater need for data use and quality improvement activities because of the ever-increasing patient enrollment into care and treatment facilities and increased programmatic demands to achieve the UNAIDS 95-95-95 goal for HIV epidemic control. Also, managers and supervisors at different levels of the health system need a system in place for timely monitoring of CQI activities for targeted technical assistance and prompt remediation on any implementation challenges. The MOHCDGEC, through the National AIDS Control Program, has a standardized tool called the Standard Evaluation System (SES) journal for documenting quality improvement activities implemented at the facility, council, or regional level. The SES form is a paper-based tool that must be filled in for each indicator being improved. The SES form allows for the documentation of CQI activities guided by the Model for Improvement developed by Associates in Process Improvement.
The Challenge
Over the years, facility CQI teams have learned how to document their CQI initiatives on the SES form, although gaps still exist. The practice varies significantly between facilities and among healthcare providers because of different levels of understanding of CQI concepts and processes. Also, because the SES form is a paper-based tool, CQI managers and supervisors have to be on-site to see what is being implemented and documented for them to mentor and build capacity on CQI. Ciheb, CDC Tanzania's CQI partner, supports CQI in more than 140 facilities in 11 of CDC’s supported regions. The team also builds CQI capacity among CDC implementing partners and regional and council health management teams.
Through this role, Ciheb has been providing technical assistance on data use for CQI through centralized training, site-level coaching, and mentorship visits through remote platforms like ECHO and Zoom. Ciheb has also managed CQI collaboratives of up to 156 facilities in efforts to improve the 95-95-95 UNAIDS goal for HIV epidemic control. Throughout this endeavor, the biggest challenge for Ciheb in Tanzania has been the timely tracking and monitoring of CQI activities across the facility, council, and regional levels. Even with the existence of multiple electronic data reporting systems in the country, none exists for CQI reporting.
Tested Change
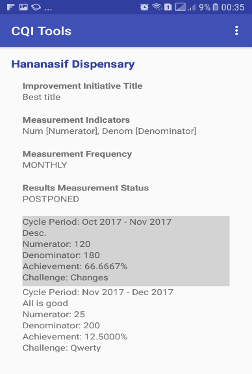
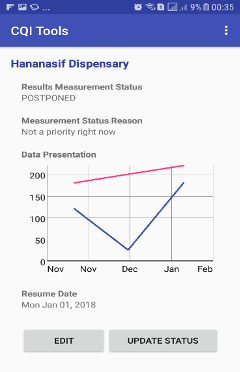
Recognizing the challenges posed by the lack of an electronic system for CQI activities, Ciheb began to develop a digital CQI reporting system through the REACH project. The endeavor began in 2017 as an Android mobile app, and in 2019, the app was complemented with a web dashboard. Both platforms mirror the SES form in the CQI reporting structure. There are two modules:
Implementation
Ciheb conceptualized, designed, field-tested, and started rolling out the CQI Android app between December 2017 and April 2018. Throughout 2018, during basic training and site-level visits, CQI teams were trained on how to use the app for documenting and tracking their CQI activities. By December 2018, there were about 513 CQI projects documented and reported by about 100 facilities from the Mwanza, Mara, Tanga, Simiyu, and Geita regions.
This process, however, faced several challenges. First, most of the CQI projects that were reported using the app did not follow the CQI process. We realized that CQI teams had a massive gap in utilizing the SES form as a paper form; thus, what was entered in the app was mostly below CQI documentation standards.
After cleaning up the reported projects, there were only about 50 CQI projects in the system that met the required CQI standards. Also, the mobile application was easy to use, depending on what type of phone the user had. The higher-end the smartphone was, the easier it was to enter data and visualize progress over time. Yet, most health providers had ordinary smartphones with tiny display screens, so this was a large obstacle.
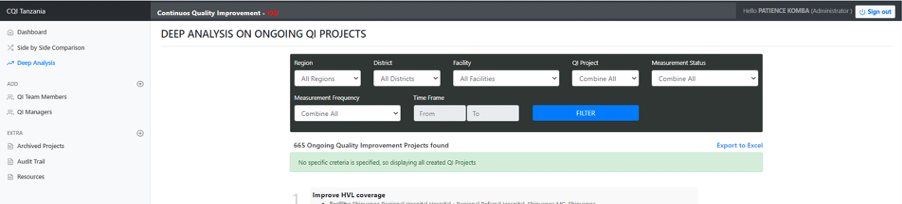
Faced with the challenges described, the Ciheb team began mentoring teams on proper documentation of their CQI activities on the SES form. We also made this a prerequisite for using the CQI application. Further, we decided to complement the CQI mobile application with the web-based platform. Facilities could choose to either use the mobile application or the web-based platform. The web-based platform ended up being much easier to use for many CQI teams. After having just 50 CQI projects in January 2019, there are now over 650 clean, well-documented, and ongoing CQI projects as of August 2020, and many more completed and archived projects.
Demonstrated Use and Impact
The digital CQI platform has progressively become more useful since its inception. Below is a summary of its advantages.

- It allows for timely monitoring of CQI activities across all levels, therefore managers can offer timely technical support either on-site or remotely.
- It allows for targeted technical assistance since managers can view facilities and their performance almost in real-time. Managers can, therefore, prioritize site visits based on what indicators are performing poorest.
- Managers can identify needs for capacity building through what the facilities are documenting. The capacity building can assist technical areas directly related to the indicators being monitored or other CQI concepts.
- The platform allows for the visualization of CQI projects and performance over time, making it easy to view multiple indicators from a single facility, councils, or regions.
- The platform comes with a CQI resources portal where all material related to CQI implementation is hosted for anyone to access freely and easily. These materials include CQI guidelines, training material, standards of procedures, and job aids.
- The platform can be used for learning and sharing of best practices either directly through its dashboard or externally using platforms such as ECHO.
The digital CQI platform also supports other functions for CQI teams at the national, regional, council, and facility level as stipulated in the Tanzania national HIV/AIDS CQI guidelines and the National CQI Framework.
At the national level
- Ensuring there is a functional CQI committee.
- Conducting operational research.
- Disseminating CQI guidelines through the resources tab.
- Providing regular support to regions in improving quality of services and monitoring its implementation.
- Identifying training needs on CQI and developing appropriate capacity building.
At the council and regional level
- Dissemination of CQI guidelines and information.
- Supportive supervision and mentoring of CQI activities.
- Evaluation of CQI activities in collaboration with regional health management teams.
- Coordinate and provide leadership in the implementation of the CQI guidelines in the region.
- Monitor and supervise the performance of districts on priority CQI targets and indicators.
- Provide regular technical support to districts in the implementation of the CQI guidelines.
- Receive district reports, aggregate, and analyze for decision making, planning, and management purposes.
- Submit reports to the national level and share with relevant stakeholders.
At the facility level
- Incorporate CQI activities for HIV and AIDS services in the health facility plan.
- Allocate resources for CQI.
- Development of organizational vision and mission statement on CQI.
- Supervise the implementation of CQI activities.
- Establish CQI team and WITs.
- Describe the roles and responsibilities of WITs and QIT.
- Collect, compile, validate, analyze, utilize, and submit timely data to the council health management teams.
Adoption and Scale-Up
Currently, the digital CQI platform has over 650 active CQI activities from 10 regions. Several facilities have shared their CQI success stories that were drawn from the dashboard in more than 30 ECHO – CQI sessions that are attended by participants from the entire country. The Tanzania National AIDS Control Program (NACP) CQI unit has adopted the CQI digital platform for tracking and monitoring CQI activities in an improvement collaborative involving three regions. Ciheb is also working with other implementing partners to scale up the use of the digital CQI platform beyond HIV/AIDS services.
The digital CQI platform is also currently used in several other Ciheb-supported countries: Rwanda, Kenya, Zambia, and Botswana.
Story by Patience Komba, Associate Director, Program Quality